
Do You use VExUS?
May 29, 2024Venous Excess Ultrasound is a grading system of systemic venous congestion. It is useful in the emergency department for patients whose fluid status is uncertain and can guide fluid resuscitation and potentially avoid systemic congestion. It is potentially useful in patients with septic shock, right heart failure or renal failure and it can be a predictor of mortality.
Classically we have used the inferior vena cava(IVC) to measure central venous pressure (CVP), given that it dilates with an increase in CVP. However it is only useful to a point, after which maximal dilatation occurs and there is retrograde pressure increase in the venous system affecting the liver and kidneys. IVC dilatation may also be falsely positive in conditions such as pulmonary hypertension.
The VExUS protocol assists in assessing the IVC and then looks at potential congestion in the hepatic, portal and renal systems.
The VExUS protocol looks at 4 areas:
- IVC diameter
- Hepatic Vein (doppler assessment)
- Hepatic Portal vein (doppler assessment)
- Infrarenal vein (doppler assessment)
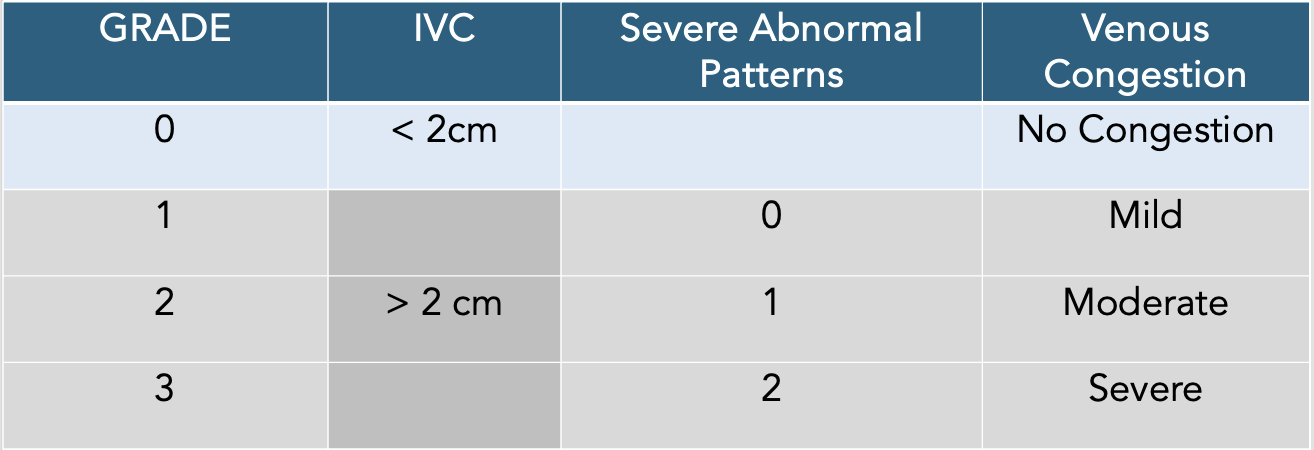
There are 4 grades depending on the level of congestion(see below).
The equipment needed is an ultrasound with pulse wave doppler capacity and either a curvilinear or phased array probe, set to abdominal or cardiac settings. The patient should be supine and have the abdominal muscles relaxed.
The probe positions are shown below:

STEP 1: Assess the IVC
Obtain a longitudinal view of the IVC as it enters the right atrium. 2cm is the landmark width of the IVC. If the IVC is < 2cm there is no congestion. If the IVC is > 2cm, then proceed to the second examination.
Assess the collapsibility of the IVC by asking the patient to take a deep breath or sniff in. The minimal diameter will be seen during inspiration and the maximal diameter during expiration. If there is COLLAPSE it means that IVC and right atrial pressures are low. The opposite will occur in ventilated patients. If IVC is < 2cm and collapses by >50% during sniff, this indicates low right atrial pressures.

STEP 2: Assess the Hepatic Vein
There are three hepatic Veins: Right, middle and left hepatic veins. Look for them as they are entering the IVC.
Place the probe in the right upper quadrant (in B mode) and then look for the veins. The 'bunny' sign may help.
Once located turn on colour to ensure that the flow is away from the probe ie., BLUE and then turn on doppler wave mode.

The doppler wave form we are looking for, is a CVP-like trace. There are three waves in the normal non-congested patient: a small positive deflection A wave and then two negative deflection waves an S and D waves. In normal vasculature the S>>D.

STEP 3: Assess the Portal vein
Place your probe in the mid-axillary line in the right upper quadrant and fan forwards and backwards. The portal vein should appear as a thick walled vessel. Once found assess with colour flow doppler. This should be RED as it flows towards the probe. Then look with pulse wave doppler.
The flow in the portal vein should be almost monophasic. When there is congestion, the flow becomes pulsatile.

Assess the severity of congestion by looking at the waveforms

STEP 4: Assess the Infrarenal Veins
The renal veins are small and may be difficult to locate. Place the probe in the right posterior axillary line. When located, turn on colour and most like both BLUE and RED will be seen.
Use pulse wave doppler. Two waveforms will appear: the arterial which is positive on the tracing and venous which is negative. Initially there is monophasic flow, however as congestion becomes more severe, it becomes a biphasic waveform and progresses to only the diastolic wave being seen.

SEVERITY Scores
References
- Rolston D et al. A higher initial VExUS Score is Associated with Inferior Outcomes in Septic Emergency Department Patients. Ann of Emerg Med. 2021;78:S82
- Qian X et al. Intrarenal Doppler Approaches in haemodynamics: A major application in critical care. Front in Physiol. 2022.13:951307
- Muthiah R. Rheumatic Mitral Valvulitis with a "Giant Vegetation" - A Case Report. Case Reports in Clinical Med. 2016;5:363-410
- Iida N et al. Clinical Implications of Intrarenal Hemodynamic Evaluation by Doppler Ultrasonography in Heart Failure. JACC. 2016;4: 674-682
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Cras sed sapien quam. Sed dapibus est id enim facilisis, at posuere turpis adipiscing. Quisque sit amet dui dui.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
